
2026 Evidence: AI in Patient Recruitment
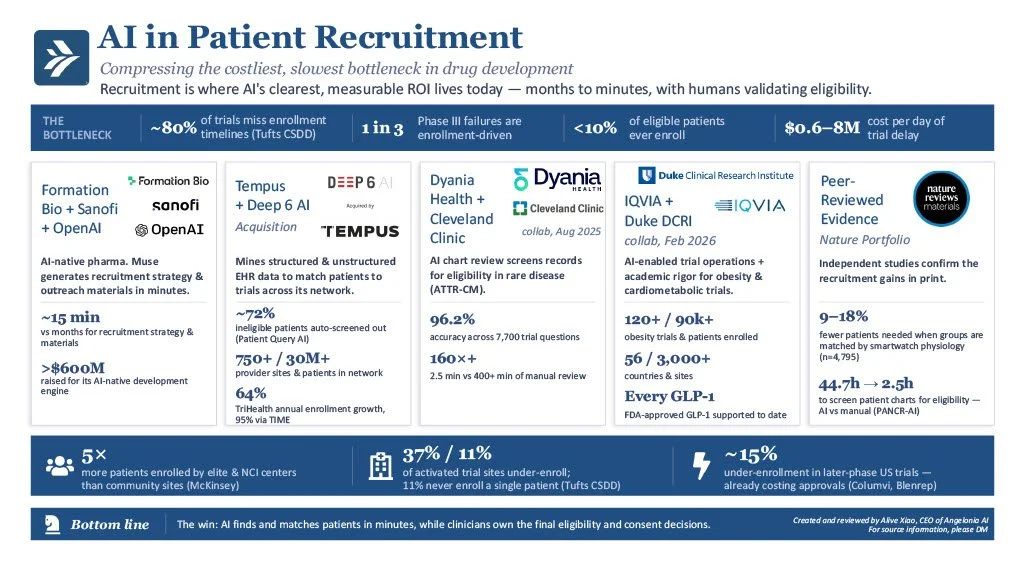
A day of clinical-trial delay can cost up to $8M, and one in three Phase III failures traces to the same quiet problem: finding patients. After years of promises, AI is finally moving that bottleneck.
The problem is structural rather than scientific. Roughly 80% of trials miss their enrollment timelines, 37% of activated sites under-enroll, and 11% never enroll a single patient (Tufts CSDD). Fewer than 10% of eligible patients ever join a trial. The patients exist — but finding them has remained a manual, chart-by-chart exercise for decades.
Across 2025 and 2026, the evidence stopped being anecdotal. Formation Bio, with Sanofi and OpenAI, built Muse to generate recruitment strategy and outreach materials in roughly 15 minutes — work that once took months. Tempus, after acquiring Deep 6 AI, now matches patients across 750+ provider sites and 30M+ records, and its Patient Query AI screens out about 72% of ineligible candidates; TriHealth credits Tempus TIME with 95% of its 64% annual enrollment growth. At Cleveland Clinic, Dyania Health's medically trained AI answered 7,700 trial-specific questions at 96.2% accuracy and read charts in 2.5 minutes versus 400-plus manually, enrolling seven rare-disease patients in six days where traditional screening had found ten in ninety. IQVIA and Duke's DCRI now bring the same muscle to obesity trials: 120+ studies, 90,000+ patients enrolled.
The peer-reviewed literature is confirming the gains: smartwatch-informed matching cut required sample sizes by 9–18% across a 4,795-person cohort (Scientific Reports), and the PANCR-AI study screened pancreatic-cancer charts in 2.5 hours against 44.7 hours of oncologist time (JMIR Cancer).
Yet the most important finding is not speed but access. Elite and NCI-designated centers enroll five times more patients than community sites, and late-phase under-enrollment of about 15% has already cost approvals (Columvi, Blenrep — McKinsey). In the Cleveland Clinic study, 36.6% of AI-identified patients were Black, against 7.1% through routine screening. AI that reads every chart finds the patients the current system misses.
For leadership teams, three disciplines apply: demand audited accuracy rather than demos, keep clinicians on the final eligibility and consent decisions, and measure what matters — screening hours saved, time-to-first-patient, and the diversity of the enrolled population.
The winners will not be the sponsors with the most recruitment vendors, but the ones who turn patient finding into a governed, auditable, continuously measured capability.
#AngeloniaAI #ClinicalAI #PatientRecruitment #ClinicalTrials #LifeSciences #ClinicalOperations #ResponsibleAI #Innovation #PharmaAI #HospitalAI